


More than 3 million people have taken the unselfish act of caring for children who are related to them but not their own biological children. These individuals are called kinship caregivers (e.g., grandparents raising grandchildren) and they often experience high levels of stress related to providing care for children. Because stress, in turn, has been associated with a number of negative health outcomes, research must focus on ways to lessen kinship caregivers’ stress to ensure their health and overall well-being. This brief will discuss financial and nonfinancial contributors to caregivers’ stress levels, the potential health consequences of stress, and possibilities for reducing stress.
Kinship caregivers may provide care under the supervision of the child welfare system (formal) or without such oversight (informal). For every child raised in kinship care in the foster care system, 18 are being raised outside of the foster care system in informal kinship. The vast majority of all kinship caregivers are grandparents, while other relatives—such as aunts, uncles, or siblings—and close family friends, including godparents or church members, make up the remainder. Approximately 63 percent of grandparent caregivers are women, 60 percent are over age 60, and 26 percent of them have a disability. Compared to their peers, kinship caregivers disproportionately experience social disadvantages: They are more likely to be single, less formally educated, unemployed, and living in poverty, placing them at significant risk for high stress levels. As a matter of fact, several research studies have confirmed that many kinship caregivers suffer from elevated levels of stress.
Among all kinship care families, Black kinship care families are overrepresented. For example, among all children living in kinship care, 26 percent are Black living in grandparent-headed households. Although stress levels are elevated for all kinship caregivers, there is reason to infer that stress is even greater among Black kinship caregivers, given that Black Americans in the general population have fewer assets to buffer stress (for example, White Americans have 9.2 times more wealth than Black Americans). Additionally, there are often differences in the support Black caregivers receive relative to White and other ethnic minority caregivers, which likely contributes to higher stress levels among this population. Ongoing racial inequities in areas such as housing, employment, and financial opportunities and resources negatively impact many Black individuals' health outcomes. These inequities likely increase the risk of chronic stress, making Black caregivers even more vulnerable.
Defining and Categorizing Stress
Stress refers to the impact of stimuli on an individual’s psychological, emotional, and physical well-being. While stress can occasionally manifest as “good stress”—such as short-term motivation or heightened alertness—it is more commonly associated with “bad stress,” which is the focus of this brief. Stress often arises from financial pressures, systemic inequities, or interpersonal and family conflicts. Stressors activate the body’s stress response system, a biologically adaptive mechanism that historically enabled humans to respond to threats by preparing for either “fight or flight.” Once a threat subsides, the body typically receives an “all-clear” signal, allowing it to return to a relaxed, balanced state known as homeostasis. However, chronic stress, an ongoing state in which the brain struggles to return to a baseline of calm, may negatively affect multiple systems in the body, including cognitive function and cardiovascular health.
Perceived versus biological stress among Black caregivers
While self-reported measures of stress offer valuable insights, they may not fully capture caregivers’ actual stress levels. A mixed-method study conducted by this brief’s first author and colleagues, which interviewed 10 Black formal and informal kinship caregivers from the Piedmont area in North Carolina, identified discrepancies between self-reported stress and biological markers such as cortisol.[1] Potentially, this suggests that caregivers may underestimate the extent of their stress. Kinship caregivers, who often face chronic stress, may become desensitized to its effects. They may normalize persistent feelings of exhaustion and being overwhelmed. Additionally, qualitative interviews with these caregivers revealed that many caregivers felt they had to keep going despite being mentally, emotionally, and physically depleted—often for the sake of the children whom they love. This normalization of stress can be dangerous to caregivers’ health, as unrecognized stress is difficult to address. Researchers should consider collecting both measures of stress—self-report and biological markers—to promote overall health among kinship caregivers.
Figure 1. Biomarker tests of Black kinship caregivers may reveal higher levels of stress than self-reports
Financial strain
A major source of kinship caregivers’ stress is financial instability, which increases vulnerability to further stress. Poverty rates are disproportionately high in kinship care families. For example, when looking at children in kinship care households where grandparents are the caregivers, about 23 percent live in households with incomes below the federal poverty level, compared to about 16 percent of all children. And, because Black individuals in the general population experience poverty at higher rates, we can infer that financial instability is likely more pronounced among Black kinship care families. Studies have also found a statistically significant relationship between family resources and stress among Black caregivers.
Many kinship caregivers assume their responsibilities suddenly—often without adequate financial, legal, or institutional support—and with little clarity about how long their care will be needed. This uncertainty contributes to chronic stress, as do housing instability, food insecurity, and lack of basic necessities. Despite federal regulations introduced in 2023 aimed at improving financial support for formal kinship caregivers, economic instability remains a key driver of chronic stress and poor health in this group—and among informal caregivers, who make up about 95 percent of kinship care families and who were not addressed in the new regulations.
Nonfinancial strains
Beyond financial stressors, kinship caregivers may also face nonfinancial challenges related to stress, including:
- Physical and emotional demands of caregiving
- Navigating complex relationships with birth parents
- Role overload from caring for multiple family members (e.g., spouse, caregiver’s parents)
- Social isolation and depressive symptoms
- Structural barriers such as:
- Difficulty enrolling children in school or accessing health care without legal guardianship
- Systems not designed for kin caregivers’ needs
- Neglect of self-care, even though it is essential for managing stress
- Recurring stressful events such as:
- Interactions with social service agencies
- Sudden school demands (e.g., preparing for testing)
- Changes in child behavior
Impact of Stress on Health Outcomes
Research indicates that long-term, ongoing stress can harm the brain and may increase the risk of disease, including Alzheimer’s disease (AD). When people are under constant stress, their bodies release high levels of stress hormones like cortisol. Over time, excess cortisol can damage the part of the brain that supports memory, contributing to the development and progression of AD. Importantly, Black individuals are two to three times more likely to develop AD than non-Hispanic White individuals. While genetics can raise a person’s risk for AD, stress is a modifiable factor that can be addressed.
Stress also negatively impacts cardiovascular disease (CVD) and has been linked to AD. The prevalence of CVD is twice as high among caregivers than among non-caregivers. Caregiver stress is associated with a two-fold increased risk of developing coronary heart disease, a 23 percent increased risk of stroke, and a 67 percent increased risk of hypertension. Additionally, CVD is more prevalent among Black individuals than among White individuals, and research has found that more Black grandparent caregivers report heart disease and other chronic conditions than their White counterparts.
Many caregivers experience a bidirectional relationship between chronic stress and CVD. Black kinship caregivers are especially vulnerable because of the combined effects of high social risk, aging, and ongoing psychosocial stress—all of which are independently associated with higher risk for CVD and AD. See Figure 2, adapted from Washington et al. (2024). One way to support caregiver health is to explore the effects of the following:
- Protective lifestyle behaviors that reduce stress and improve health
- Maladaptive coping strategies and barriers that prevent engagement in health-promoting behaviors
Figure 2. The influence of positive lifestyle behaviors and modifiable risk factors on Alzheimer’s disease
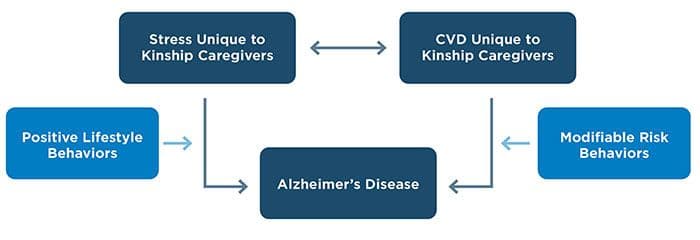
Source: Adapted from Washington, T., Coley, S., Blakey, J., Downing, K., Lewis Wallace, Q., Levkoff, S., & Cook, B. (2024). Conceptual framework for African American kinship caregiver’s susceptibility to Alzheimer’s disease. Healthcare, 12(23), Article 2379. https://doi.org/10.3390/healthcare12232379
Opportunities to reduce AD risk in Black kinship caregivers
By listening to and partnering with Black kinship caregivers and families, and by leveraging both new and existing protective community resources, we can address chronic stress, lower the risk of CVD, and reduce the likelihood of AD. These efforts can strengthen not only caregivers’ health but also the well-being of the children for whom they care, and for the entire family unit.
Engage and listen to Black caregivers.
- Ask caregivers directly about their needs and preferences and solicit their ideas for reducing stress and improving health.
- Explore questions with caregivers such as:
- Would peer support groups be helpful for you?
- What should respite care look like in your community?
- Do you have opportunities to attend church or other social groups that provide emotional and spiritual support?
Integrate culturally relevant services and interventions.
- Many Black families do not use the term “kinship care” and instead describe their caregiving using language such as “raising my grandkids” or “helping out family”; some never distinguish between raising related children and their own biological children. When conducting outreach to provide services or support to these families, it is important to use language they are familiar with so they know these resources are there for them.
- Ensure that programs and services designed to support the needs of kinship caregivers and families are effective for all. For example, if Black caregivers are more comfortable attending school supply giveaways in the communities where they live, then organizations should host such events locally to increase participation.
- Kinship care has long been a cultural asset in the Black community, serving as a source of strength and resilience across generations.[2],[3] For example, historically, this kind of family structure supported children during the era of slavery and the Great Migration, and when Black communities were increasingly (and disproportionately) affected by incarceration (e.g., War on Drugs, prosecutorial racial disparity). Recognizing the deep-rooted strength of kinship care can help reduce the stigma sometimes associated with it and inform supportive practices.
Leverage protective community resources.
- Build on existing community strengths such as extended family networks, faith-based organizations, and social groups.
- Support the creation of new resources that are designed or co-designed by community members.
Promote behavior changes that reduce risk.
- Provide caregivers with safe and affordable opportunities for exercise, healthy meal preparation, and other self-care practices.
- Reduce daily stressors by connecting caregivers to programs that help them navigate school systems, health care, and financial assistance.
Summary
Black kinship caregivers take on the selfless responsibility of providing love, support, and care to children who are related to them, but not their own biological children. However, the demands of caregiving can increase caregivers’ stress levels due to both financial and nonfinancial factors. Fortunately, Black families and communities possess many strengths that can serve as powerful protective community resources, helping reduce stress and ultimately lower caregivers’ risk for AD and other health problems. Child welfare leaders and programs should utilize these protective community resources to expand or develop culturally relevant preventions and interventions and health services that improve Black kinship caregivers’ stress levels and reduce their risk for AD. These interventions and services not only have the potential to improve caregivers’ immediate and long-term health outcomes, but also the well-being of the children they care for, as recent research indicates that lower caregivers’ stress levels have a positive influence on children's outcomes, including mental health.
Suggested citation
Washington, T., & Martinez, D. N. (2025). Prioritizing Black kinship caregivers’ health means reducing their stress. Child Trends. DOI: 10.56417/6730w6505z